Studia z Polityki Publicznej
ISSN: 2391-6389
eISSN: 2719-7131
Vol. 9, No. 2, 2022, 9-30
szpp.sgh.waw.pl
DOI: 10.33119/KSzPP/2022.2.1
Usman W. Chohan
Centre for Aerospace & Security Studies (CASS), Islamabad, Pakistan, e-mail: usman.chohan@csa.org or uchohan2@gmail.com, https://orcid.org/0000-0001-8915-8290
Analyzing sound COVID-19 policy responses in developing countries: the case study of Pakistan
Abstract
The COVID-19 pandemic has posed significant policy challenges in developing countries, where operational resources and policy capacity are limited. Yet, some developing countries have fared better than others, and part of this success seems to be attributable to the use of prudent policy instruments within a policy mix that exhibits coherence. This article presents a COVID-19 case study of Pakistan and considers the following aspects of Pakistan’s policy mix: (1) polio and rural support infrastructure deployed for COVID-19 detection and awareness-creation; (2) the establishment of a national command and operation center (NCOC) to centralize real-time decision-making; (3) the use of the largest income support program to generate a targeted pro-poor stimulus; and (4) optimally targeted (smart) lockdowns. The findings suggest that developing countries can adjust sound policy responses to pandemic conditions despite their resource constraints, by calibrating extant policy instruments and mobilizing new ones within a coherent policy mix.
Keywords: COVID-19, pandemic, policy response, developing countries, public value, Pakistan, policy mix, policy instruments
JEL Classification Codes: D73, H83, I15, I18, J18
Analiza dostosowania polityk publicznych w reakcji na COVID-19 w krajach rozwijających się. Studium przypadku Pakistanu
Streszczenie
Pandemia COVID-19 postawiła duże wyzwania polityczne przed krajami rozwijającymi się, w których zasoby operacyjne i możliwości polityczne są ograniczone. Jednak niektóre z tych krajów radzą sobie lepiej niż inne i wydaje się, że część tego sukcesu można przypisać wykorzystaniu ostrożnych instrumentów polityki publicznej w ramach spójnych kombinacji interwencji publicznych. W niniejszym artykule przedstawiono studium przypadku dotyczące pandemii COVID-19 w Pakistanie i rozważono następujące aspekty kombinacji polityki publicznej: 1) polio i infrastruktura wsparcia obszarów wiejskich wdrożona w celu wykrywania COVID-19 oraz budowania świadomości na ten temat; 2) utworzenie krajowego operacyjnego centrum dowodzenia w celu scentralizowania procesu decyzyjnego prowadzonego w czasie rzeczywistym; 3) wykorzystanie największego programu wspierania dochodów do zorganizowania pomocy dla ubogich; 4) optymalnie ukierunkowane (inteligentne) lockdowny. Wyniki badania sugerują, że kraje rozwijające się – pomimo ograniczonych zasobów – mogą odpowiednio zareagować na pandemię poprzez dostosowanie istniejących instrumentów politycznych i stworzenie nowych w ramach spójnej kombinacji polityki publicznej.
Słowa kluczowe: COVID-19, pandemia, reakcja polityczna, kraje rozwijające się, wartość publiczna, Pakistan, kombinacja polityki publicznej, instrumenty polityczne
Kody klasyfikacji JEL: D73, H83, I15, I18, J18
The sudden outbreak of the novel coronavirus (COVID-19) pandemic caught the global public unaware in late 2019 and early 2020, with many countries finding their existing public health infrastructure and operational resources pushed to the limits by the rapidity of its contagion. Although scientists had long been cautioning governments to prepare for severe infectious disease outbreaks (see Anthony et al., 2017), the coronavirus pandemic tested the mettle and preparedness of all countries (Capano et al., 2020), thus presenting public managers around the world with a formidable challenge in terms of preserving both lives and livelihoods (Chohan, 2020a, 2021). However, the pressure that the pandemic exerted on public managerial infrastructure was more pronounced in developing countries where policy expertise (Singh & Misra, 2020), social protection (Gerard et al., 2020), and overall policy capacities were far more constrained (Hussein et al., 2020; Chohan, 2020b).
As Rasul notes, “all countries are challenged, but low-income and developing countries are facing a more challenging situation than others” during the COVID-19 pandemic, which he attributes to “their limited health infrastructure, limited financial and human resources, low human capital, and limited capacity of governments to respond” (2020: 59). Given this dire situation, the grim outlook was that developing countries might well confront catastrophic economic and public health outcomes, as indeed Brazil and India did (Figure 1). Yet, some developing countries have (thus far) fared considerably better than others, both in terms of rebounding economic activity as well as suffering fewer numbers of cases and deaths (Chohan, 2020c). It would appear, in fact, that some developing countries have even fared better than many developed ones in these terms (Figure 1).
Figure 1. Cumulative COVID-19 deaths in four large countries
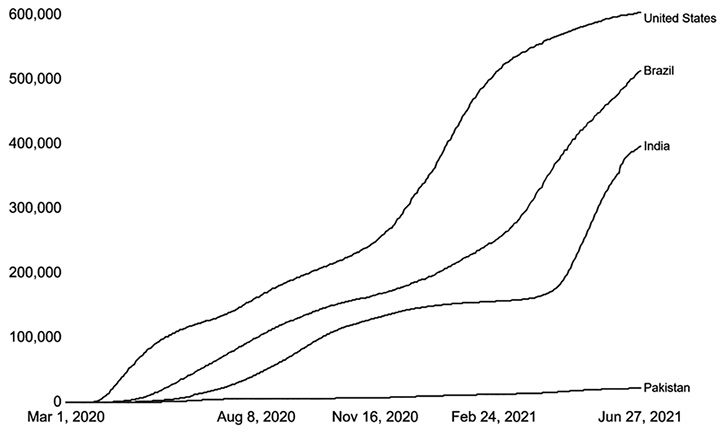
Source: Johns Hopkins University Coronavirus Research Centre (2021). As of June 29, 2021.
Part of this success seems to be attributable to the integration of prudent policy instruments within a policy mix that exhibits coherence and complementarity. As Rasul advised for such countries, “with weak health infrastructure and limited financial and human resources, strategic thinking and planning and setting priorities for policies and activities [would] be critically important for developing countries to manage COVID-19 challenges” (2020: 60).
Thus, the aim of this article is to explore how developing countries have mustered sound public policy responses to pandemic conditions by adjusting and calibrating operational resources and instruments within a coherent policy mix (see policy mix in Chapman, 2003; Hennicke, 2004; Howlett & Del Rio, 2015; developing country public policy in Osman, 2002). It relies on a policy-instrument approach (Howlett, 2005), which is justified, as Capano and Howlett argue, because “an instrument-based approach can better enlighten the nature of policy dynamics, from a prescriptive point of view, and assist policymakers in taking more effective decisions than can a purely input-based approach” (Capano & Howlett, 2020).
The article builds on a case study of Pakistan, which is a notable success story in the early phase (2020–21) of the COVID-19 pandemic (Figure 1), with only 22,000 deaths as of late June 2020 for a country of 220 million people, and year-on-year GDP growth of 3.9% for the fiscal year 2021 (July 2020–June 2021). Some scientists have described its success as “puzzling” (Shah & Xing, 2020: 92), but a public policy lens that identifies the salient policy instruments within a coherent mix, and looks at the effective calibrations in policy implementation, might dispel some of that mystification. Indeed, as The Economist reported in its first Global Normalcy Index, Pakistan ranked third in the entire world, behind only New Zealand and Hong Kong, in terms of the degree to which it attained pre-pandemic levels of normalcy (The Economist, 2021), which is remarkable for a developing country.
Table 1. Selected policy elements in Pakistan’s COVID-19 response
|
Policy problem |
Policy instrument/strategy |
Category of policy action |
|
COVID-19 detection, awareness-creation, inoculation |
Redeploy polio workers’ network and Rural Support Program (RSP) networks for COVID-19 detection, awareness campaigns, and inoculation |
Policy recalibration from the existing system for a special project |
|
Disparate/fragmented command |
Centralizing the response through a national “nerve center” (NCOC) |
Centralization of decision-making that integrates multiple stakeholders |
|
Income protection |
Use the country’s largest income support programs (BISP/Ehsaas) to identify needy households and disburse relief funds |
Policy recalibration from the existing system towards a special project |
|
Balancing lives vs. livelihoods |
Smart lockdowns: targeted measures to close down specific hotspots without shuttering entire communities/cities |
Targeted implementation of best practices in the local context |
Source: own elaboration.
Towards that end, the article considers four instruments within Pakistan’s overall policy mix: (1) polio and rural support infrastructure redeployment; (2) the establishment of a national command and operation center (NCOC) to centralize decision-making; (3) the use of the largest income support program to generate a targeted pro-poor stimulus; (4) and optimally targeted (smart) lockdowns. These are also enumerated in Table 1. All four policy instruments were crucial contributors towards Pakistan’s public value preservation, but they each addressed different policy problems and relied upon varying categories of policy action. The policy problems they sought to address were common in the developing world, and on occasion, also resonated with the circumstances of some developed countries as well, as follows: ensuring COVID-19 detection; fragmented or disparate institutional landscapes; launching income protection programs and choices in balancing lives vs. livelihoods.
It is such a policy mix and its diversity of instruments, the article argues, which coalesced (and was integrated) into a coherent policy response to the pandemic by tackling both the economic and public health fallout of the COVID-19 outbreak. To present a case study that places each of the four instruments selected for this article in the proper context, the structure of the remainder of the article is as follows. Firstly, it conducts a select review of the public policy literature as it pertains to policy mix, policy capacity, and policy coherence, insofar as they apply to the challenges faced by developing countries in pursuing an effective policy response during the pandemic.
Secondly, the article builds upon the four policy instruments mentioned in Table 1 as the crux of the case study that considers the nature and the application of various policy instruments. On this point it should be noted that the four instruments examined in this article are by no means the sole elements of Pakistan’s strategy, and it is also important to remember that the link between policy instruments and outcomes is indirect as well as limited (Koontz & Thomas, 2012). For example, as Shah and Xing note, Pakistan undertook other “rigorous measures, including: establishing special hospitals; testing laboratories and quarantine centers; providing treatment; increasing public awareness; and ensuring the emergent response of local communities” (2020: 92), and these are not the object of analysis in this article but warrant recognition at this juncture.
In that sense, the scope of the article is limited in that it covers a select contingent of policy instruments integrated within a policy mix that is of particular interest because they addressed policy problems of the scope beyond mere conventional public health interventions, such as centralization of public policy, smart lockdowns, and income support (but see also public health and immunology discussions in Khalid & Ali, 2020; Peter et al., 2021). Thereafter, and thirdly, the article presents a brief discussion that analyzes the impact of these policies on Pakistan’s overall COVID-19 policy mix, especially in terms of building policy coherence, thereby exemplifying how developing countries might adjust solid responses to the pandemic and other crisis contexts despite resource constraints. The final section presents concluding remarks wherein certain limitations of the research are also considered.
Public policy challenges of developing countries in the pandemic
The public policy literature tends to agree that a thorough and wide-encompassing policy response, and one that prudently incorporates different policy goals and instruments, is a necessity for tackling large-scale exogenous crises (see Ansell et al., 2010), such as the COVID-19 pandemic (Ansell et al., 2020). There are many different lenses from within the public policy literature that can be mobilized towards understanding COVID-19-related national responses, including policy integration (Tosun & Lang, 2017), policy coordination (Peters, 2015), and policy mixes (Howlett & Rayner, 2007), among others, and focus of this article is on select policy instruments within a policy mix.
The notion of policy mix is used frequently in the literature to analyze systematic policy responses that deploy various instruments in combinations (Chapman, 2003; Hennicke, 2004). The literature reasons that the necessity and reality of multilevel governance (i.e., at varying levels of government authority) require policy actors to contend with different policy means and ends (Howlett & Del Rio, 2015), because of which a policy mix emerges. The primary aim of an effective policy mix is to extract synergies, which are seen through the arithmetic representation of 1 + 1 ≥ 2 (Mei, 2020). This speaks to Daugbjerg’s contention on policy design, thinking that policymakers must maximize complementary effects (and minimize conflicting effects), while policy mixes are deployed (Daugbjerg, 2009).
Yet, integrating different policies may not translate automatically into a coherent policy mix, particularly if the goals and instruments do not support one another (Trein, 2017). The policy instruments chosen in this article may seem disparate or in disjuncture, but this article argues that they fit with a degree of coherence in an overarching policy mix (see also Table 1). For example, the polio and rural support infrastructure (instrument #1) and BISP records (instrument #3) compiled district- and area-level data for each province, which was transferred on a daily basis to the centralized NCOC (instrument #2), which then made decisions about smart lockdowns (instrument #4). This is expressed diagrammatically in Figure 3.
To attain synergies, divergent policy instruments must be integrated into a coherent policy program (Trein & Maggetti, 2020) that can reach across policy sectors (Howlett & Rayner, 2007; Knill et al., 2021). In Pakistan, the instruments used were guided by an overarching policy framework known as the National Action Plan for the Corona virus disease (COVID-19) Pakistan (Ministry of National Health Services; MNHS, 2020). Instruments in the policy mix can have interactive effects among them and can be considered consistent or complementary when they work together to support a policy strategy (Kern & Howlett, 2009; Rogge & Reichardt, 2016). But there is much caution found throughout the policy design literature that not all tools are inherently complementary (Del Río et al., 2011; Grabosky, 1995). If designed poorly, in the sense of conflicts among the underlying policy instruments within the mix, the result may well be policy incoherence (May et al., 2006) or policy inconsistency (Howlett & Rayner, 2007).
Yet, policy mixes during crisis conditions should be different from those in normal conditions (Yang, 2020). Periods of crisis may compel public managers to adopt multiple policy instruments in a potentially hasty or excessive manner (Maor, 2019) but such are the pressures of taking timely decisions during fast-changing circumstances (Adolph et al., 2021). In crisis contexts, an important form of policy action is to calibrate (or recalibrate) existing instruments towards new policy goals. Calibrations are defined by Capano and Howlett as “those contextual actions and decisions through which policymakers adjust the actual setting of policy instruments with respect to the target of interest” (2020: 9). Calibrations are seen as “the order of the day in policymaking, especially in the implementation stage when policies need to be delivered in an effective way” (Capano & Howlett, 2020: 9; see also Hall, 1993).
This article argues, especially through instruments #1 (polio infrastructure) and #3 (income protection) that the success of developing countries in confronting crisis conditions such as the COVID-19 pandemic can be realized through recalibrating the limited policy capacity and operational resources that they possess. The literature argues that a prudent policy calibration “requires continuous managerial attention to the social and political environments, and adaptation of current decisions to new social concerns” (Preston & Post, 1981: 57). The degree and nature of calibration will also depend on the instrument and on its position within the policy mix, and they “feature the use of combinations of different kinds of policy tools … whose exact configuration changes from location to location” (Rayner et al., 2017: 473).
Yet one issue that mars the ability of developing countries to grapple with crisis conditions is the deficiencies of policy capacity (Davis, 2000), defined as “the set of skills and resources – or competences and capabilities – necessary to perform policy functions” (Ramesh et al., 2015: 166). This also correlates with the absence of resilience and robustness in public policy design (Capano & Woo, 2017; Dimian et al., 2017), which have been and are being tested by the stresses of COVID-19. It is also exacerbated by the effects of policy myopia (see Nair & Howlett, 2017).
Although publications regarding public policies, as well as social policies (see the distinction in Błędowski, 2014), in pandemic-related crisis-contexts have mushroomed since COVID-19 was declared a global pandemic by the WHO in early 2020, much of this research examines the developed world’s context. Much of the focus is on the absolute and relative intensities of the crises that they faced (South Korea in Lee et al., 2020; Singapore in Woo, 2020), the legitimacy that public managers enjoyed or lacked (Hong Kong in Hartley and Jarvis, 2020), and the degree of policy customization and mix that they employed (China in Mei, 2020; Canada in Migone, 2020; the US in Rocco et al., 2020). The developing world is somewhat under-represented in the contemporary wave of research, and this gap can be addressed through useful case studies of the developing world’s context, a point to which the enquiry of this article speaks.
Case study: select instruments in Pakistan’s COVID-19 policy mix
As with all other countries, the onset of COVID-19 served as a disruptive exogenous shock that threatened both lives and livelihoods, but what made Pakistan’s conditions different was that its economy had already been struggling before the pandemic even began (Ashfaq & Bashir, 2020; Chohan, 2020b). Whereas most Asian countries had been estimating reasonable growth prior to the pandemic’s eruption, Pakistan was already mired in stagflation conditions where prices were rising for consumers, but economic activity was failing to grow. As such, the State Bank of Pakistan (SBP) Governor Baqir feared that growth could fall below 3.5% in the fiscal year 2020, and the IMF’s forecast for that year was of an even lower 2.4%., and that, too, for a population growing at roughly 3% per annum (see Ahmed, 2020).
Other social factors also presented an ex-ante fear of contagion risk in Pakistan, including illiteracy insofar as it impacted social compliance with any necessary restrictions (see compliance in Grabosky, 1995), social media misinformation (Ittefaq et al., 2020), the lack of social protections (Syeda, 2015), work precarity (Chohan, 2020b), and the lack of participatory allocation of resources (see participatory budgeting in Pytlik, 2017). Furthermore, healthcare infrastructure was already deficient in Pakistan (Hassan et al., 2017), and budgetary allocations as a percentage of GDP had always been very low in the country (Hafeez, 2014). As Byszewski points out, the laws that govern public healthcare provision are important in assuring better public health outcomes (2018), but the general assessment of the implementation of these laws in Pakistan was characterized by a deficient implementation (Hafeez, 2014; Hassan et al., 2017).
In addition, as the public policy literature highlights in terms of the importance of public managerial legitimacy (Chohan, 2019; Howlett, 2019), Pakistan’s state legitimacy was typical of a developing country and thus constrained in securing the “authorizing environment” (Moore & Khagram, 2004: 8) requisite for public value creation. According to the Global State Legitimacy Index (GSLI), Pakistan had a score of 7.6/10, comparable to Zambia, Lebanon, or Bangladesh (GSLI, 2021), but had improved from a rank as low as 8.6 in 2009. Each of the foregoing challenges is enumerated in Figure 2.
Figure 2. Ex-ante challenges in Pakistan
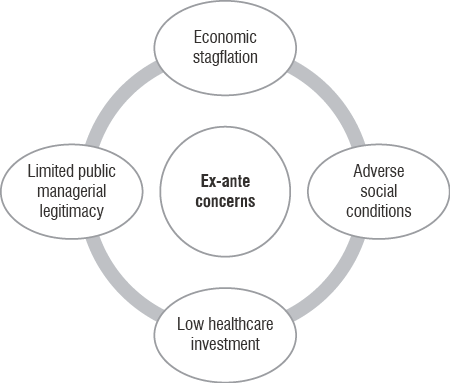
Source: own elaboration based on GSLI (2021); Ittefaq et al. (2020); Syeda (2015); Chohan (2020b); Hafeez (2014); Hassan et al. (2017); Ahmed (2020); Ashfaq and Bashir (2020).
This meant that were a global pandemic to hit the prognostications of Pakistan’s ability to pursue an effective policy response were grim. For example, an algorithm designed at Imperial College London in early 2020 predicted that, in a worst-case scenario, Pakistan would suffer 79,000 deaths by August 10, 2020; and if left entirely unchecked, by January 26, 2021, the death toll would reach an astounding 2.3 million (Mangwat, 2020). The same algorithm predicted that by January 26, 2021, the total death toll would be a colossal 14,244,379 without intervention (Mangwat, 2020). Yet, such a grim ex-ante foreboding did not come to pass (Figure 1), and the four selected instruments within the policy mix that Pakistan deployed offer some explanation and lessons for developing countries in that regard.
Instrument one: networks – the polio and rural support infrastructure
Pakistan is one of the few countries in the world where the polio virus still exists, and the policy capacity in Pakistan has, despite political will and international support, not eradicated the virus altogether, particularly due to its prevalence in Afghanistan, whose porous border with Pakistan brings and breeds the wild polio strain (Yusufzai, 2020). However, an existing architecture for polio detection and inoculation has been built in Pakistan over the past few decades, involving civil society volunteer work and a Rural Support Program (RSP) network as well (RSP, 2020). This speaks to the recognition of active civil society participation in policy implementation (Legutko-Kobus, 2018), as the RSPs would deploy individuals, sometimes at great personal risk (Abimola et al., 2013), to pursue polio vaccination in remote and economically backward areas of the country. The structure of RSPs was such that they were present in 149/156 districts of Pakistan and mobilized over 8.4 million rural households (equivalent to roughly 54 million individuals) into a network of 498,200 community institutions (RSP, 2020).
The RSPs offered a latent policy instrument that could be mobilized towards COVID-19 detection, awareness-creation, and even vaccination. Thus, Pakistan recalibrated the policy instrument to target COVID-19 detection in rural communities. As the RSP network reports, they have been actively working during the pandemic on an anti-COVID-19 response in 126 of the country’s districts, often in particularly underdeveloped areas (RSP, 2020). The RSPs are also fulfilling that gap identified in the literature of multilevel governance, because they are “facilitating links between government and rural communities” and sit on “numerous provincial, district, tehsil [sub-district], and union council committees,” (RSP, 2020).
For awareness-creation, the RSPs have been disseminating critical messages to communities regarding the essential precautionary measures, including social distancing, hand washing and hygiene measures, and self-isolation protocols. This is important due to the low level of literacy in the country at only 60% (70% for men, 50% for women, see O’Neill, 2021), such that social media and government announcements would not necessarily or easily reach all communities. Furthermore, community institutions, community activists, and dissemination tools (loudspeakers, banners) have supplemented the polio infrastructure.
The World Health Organization (WHO) recognized the use of the polio eradication instrument for COVID-19 purposes and stated that “polio teams in Pakistan have been working to support the COVID-19 response since the beginning of the pandemic, as well as continuing with their work to eradicate polio” (WHO, 2020b). The WHO noted that the polio infrastructure “has adapted existing acute flaccid paralysis (AFP) surveillance networks embedded in hospitals and health facilities to detect COVID-19 as well as polio,” and that polio workers “have been helping with testing and have trained health workers on infection prevention and control” (WHO, 2020b). Meanwhile, polio “data management systems across the country and a call center in the Capital, Islamabad, assist in addressing misinformation and helping to detect suspected COVID-19 cases” (WHO, 2020b).
Instrument two: the National Command and Operation Centre (NCOC)
Policies have a procedural component which consists of the processes or activities relating to coordination of policy actors who engage in formulation, decision-making, and administration (Howlett, 2011). As Dudzińska highlights, there are perennial public policy implementation problems that hamper, particularly at the earlier stages, the ability of key stakeholders to realize public policy outcomes as they are initially intended (2015). This problem is all the more acute in developing countries because of fractured governance mechanisms and institutional weaknesses, a point raised in the earlier literature review, which is no less true of Pakistan. Public health experts were arguing that developing countries should “establish a cross-sectoral coordination body,” since “a multi-sectoral coordination body can provide an effective pathway for engaging multiple stakeholders,” while also offering “the basis for a mechanism for coordinating and steering the decision-making process and overseeing the implementation and recovery packages to maximize impact” (Rasul, 2020: 59).
With this in mind, the government of Pakistan adopted a centralizing mechanism for real-time decision-making during the COVID-19 pandemic known as the National Command Operation Centre (NCOC). As Shah and Xing observe, the government of Pakistan established the NCOC “to formulate and implement a comprehensive strategy to stop the spread of SARS-CoV-2” (2020: 92). According to the NCOC’s own definition, it was “the nerve center to synergize and articulate unified national effort against COVID-19” (NCOC, 2020; see also MNHS, 2020). It considered itself a “one window operation to collate, analyze, and process information based on digital input and human intelligence across all [of Pakistan]” (NCOC, 2020). The NCOC has a multistakeholder composition of public health officials (including those with WHO experience), high-level political representatives, civil and military experts, along with provincial representatives.
The NCOC has relied on “a well-structured IT-based national framework for credible health resource mapping” that covers 4,000 hospitals and health centers across the country, along with inputs from the polio network and rural support programs (see instrument 1 in this section). The NCOC is also bolstered by an Integrated Disease Information Management System (IDIMS), which integrates all real-time data from the field and serves as a repository for data analytics such as disease projections and the identification of targets for smart lockdowns (see also instrument 4 in this section).
As such, while acting as the centralized nerve system of the pandemic response in Pakistan, the NCOC could address issues in hot spots across the country in a data-driven and rapid manner. It was, therefore, instrumental in minimizing the damage to lives and livelihoods throughout the pandemic by taking inputs from other policy instruments (e.g., instrument #1: polio infrastructure, and instrument #3: income support program) to give calculated decisions as outputs to other instruments (e.g., instrument #4: smart lockdowns). This is expressed diagrammatically in Figure 3.
Instrument three: Income Support Program
Pakistan is a society marred by considerable income inequality (Safdar & Chohan, 2020), and as Ashford et al. observe, socioeconomic inequalities became more pronounced in the wake of the COVID-19 pandemic (2020). Nearly all countries undertook Keynesian stimulus programs (see the analysis in Chohan, 2022), but Pakistan’s constrained fiscal space meant that it had to maximize the pro-poor impact of any stimulus that it undertook. Ultimately, the government’s early-phase pandemic stimulus amounted to $ 5 billion dollars, or 2% of GDP, which was much lower in absolute and relative terms than even many developing countries (see IMF, 2020; Chohan, 2020a-c). Yet the key question was how to determine who was most deserving of the COVID-19 relief funds: a seemingly daunting identification-problem for a country of 220 million people.
For this purpose, the government recalibrated the existing policy instrument of the Benazir Income Support Program (BISP), along with its merger into the current government’s Ehsaas welfare program. This was a recommendation of the Asian Development Bank, “considering the comparative advantage of using [its] existing and well-established implementation arrangements” (ADB, 2020). The BISP was created as an unconditional income cash transfer program in 2008 and was intended for the most destitute elements of society, transferring roughly 2,000 rupees (roughly $ 13 USD) per month to 4.5 million households through the women of the household. As Pakistan’s largest safety net institution, the ADB remarked that the BISP had “established policies, systems, and procedures, with demonstrated capacities in… the social protection of the poorest segments of society” (ADB, 2020: 14).
Recalibrating this policy instrument allowed the government to target the neediest in society and, therefore, maximize the value of the stimulus program. This was markedly different from several developed countries such as the US, which could (1) print unprecedented stimulus sums (see Chohan, 2020d), and (2) much of the stimulus was gobbled up by corporations and large private interests rather than by the poor (see Whoriskey et al., 2020). The BISP also served as a source of data inputs into the NCOC (see instrument #2) as its data also helped reveal the intensity of the pandemic at regional-specific levels of analysis.
The disbursements issued through the BISP to the neediest households meant that the poor in the country could withstand the recessionary environment of the pandemic without succumbing to desperation and without needing to struggle (with undue delays) to justify their needs-based qualification for assistance. As such, the recalibration of the Ehsaas/BISP towards pandemic relief served as a policy input for decision-making, but also as an output for pro-poor stimulus and income support (see also Figure 3).
Instrument four: smart lockdowns
Many countries took extreme measures in the lives vs. livelihoods tradeoff (see Chohan, 2020a) by either shutting-off entire sections (or the whole) of the economy, or by letting things continue in an entirely business-as-usual fashion (see discussions in Lee et al., 2020; Woo, 2020; Hartley & Jarvis, 2020; Mei, 2020; Migone, 2020; Rocco et al., 2020). By contrast, Pakistan adopted a “third-way approach” (Chohan, 2020c), which involved the usage of smart (targeted) lockdowns. Although many studies have been published regarding optimal lockdowns in the COVID-19 pandemic (see Fu et al., 2021; Bosi et al., 2021), the question of optimality in lockdowns and quarantines has long been studied in the epidemiology literature (see reviews in Sharomi & Malik, 2017; Shi & Tan, 2012). This literature helped to inform the epidemiologists who were part of the NCOC, including those with WHO experience; and as such, international best-practices and lesson-drawing in public policy were applied to the local context (see also Dolowitz & Marsh, 2000.)
This policy instrument relied on the identification of hotspots by the NCOC (instrument #2) based on grassroots-level data inputs from hospitals and other instruments such as RSPs (instrument #1, #3). Although smart lockdowns were identified by the NCOC, the approach itself exemplified multilevel governance (see Szarfenberg, 2015) in that it required the coordination of central, provincial, district, and municipal levels of coordination to close-off effectively targeted locations. Various authors have analyzed the merits of Pakistan’s smart lockdown approach (Ghaffar et al., 2020; Ghaffar et al., 2021; Saeed et al., 2021) and rendered a positive verdict on the policy instrument. For example, Ghaffar et al. highlight that the smart lockdown could “show long-term results needed for controlling COVID-19 without creating any major disturbance in the economy” (2020: 32), and various models point out the relative efficacy of the smart-lockdown approach in striking an adequate balance (Ghaffar et al., 2020), so long as they are targeted carefully and implemented effectively (Saeed et al., 2021).
The imposition of a targeted lockdown was carried out with strict orders and the threat of punishment that was enforced by civil and military mechanisms (Saeed et al., 2021), which meant that the efficacy of identification was backed with the coherence of oversight and enforcement on the ground (see Walby, 2013). Hence, Pakistan was able to deploy a policy instrument that balanced the dual goals of keeping the overall economy going and keeping the cases and deaths from COVID-19 low.
Was the policy mix coherent?
Given the foregoing discussion, it is worth examining whether coherence was manifested in Pakistan’s COVID-19 policy mix and whether synergies were extracted. Rasul noted in the context of the early phase of the pandemic that “there are many areas where improving policy coherence and coordination can reduce trade-offs and improve synergies and thus increase the net positive gain to society” (Rasul, 2020: 59). Figure 3 demonstrates the policy coherence in Pakistan’s pandemic response. At the initial stage of the pandemic, the government of Pakistan decided to centralize command through the NCOC, which would consist of multistakeholder membership and would apply data-driven approaches to decision-making. These decisions would be informed by networks including RSPs, the polio infrastructure, hospitals, health centers, and other sources. These sources would reinforce one another and give a real-time picture of the hotspots as they emerged around the country.
Informed by the field data, the NCOC would identify targeted locations for smart lockdowns, which would be enforced through various civil and military institutions. The objective of minimizing the number of cases and deaths while also minimizing the economic paralysis of the pandemic was thus met with a largely coherent approach, using compatible options and in a mutually reinforcing manner.
Figure 3. Policy coherence in Pakistan’s pandemic response
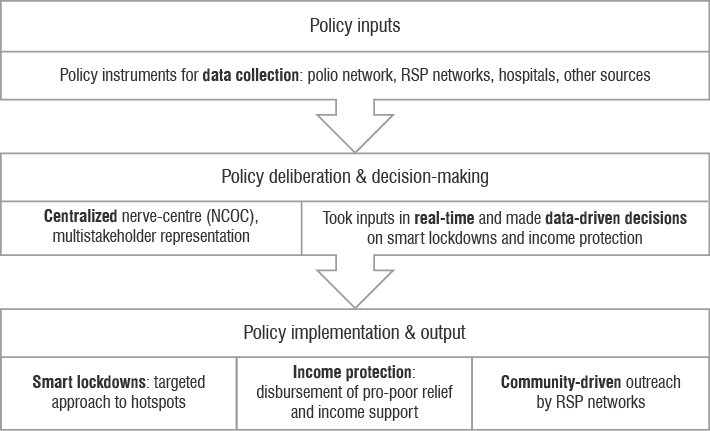
Source: own elaboration.
***
Developing and developed countries alike confronted an exogenous shock of COVID-19, which hurled them into a period of uncertainty. Developing countries faced particularly dire ex-ante circumstances, as exemplified by Pakistan’s pre-pandemic stagflationary environment, limited public managerial legitimacy, and several other adverse social conditions (Figure 2). Yet, as mentioned earlier, Pakistan ranked third in the entire world in The Economist’s first Global Normalcy Index, behind only New Zealand and Hong Kong (2021), which sets it quite apart from other developing countries, and which was seen as a “puzzling” feat (Shah & Xing, 2020: 92). The foregoing analysis of the policy mix, however, sheds some light on the “puzzling” success that Pakistan achieved, where the foregoing four instruments helped to play a key role, although not an exclusive one, since, as Capano and Howlett have remarked, “more research is needed to order the complex world of mixes and, above all, to disentangle how different factors drive the design of good or bad policy mixes” (2020: 3).
As Howlett has commented, policymakers are always “responding to a whole host of social, political, economic, and administrative concerns when selecting a particular technique by which to obtain their policy goals” (1991: 1). This is why several limitations to the research in this article warrant mentioning. Firstly, the pandemic has yet not ended as of this writing, and in Pakistan, a possible “fourth wave” might yet occur with the Indian (Delta) variant at its vanguard. Secondly, this article considered four important policy instruments, but this did not constitute the entirety of Pakistan’s policy mix; however, it is important to remember that the link between policy instruments and outcomes is indirect as well as limited (Koontz & Thomas, 2012). Pure and direct healthcare interventions, for example, have not been covered in this article but have been studied at length elsewhere (Khalid & Ali, 2020; Peter et al., 2021) and would go beyond the scope of a single article.
Furthermore, lessons from Pakistan’s context may not apply directly to all developing countries (e.g., polio infrastructure). Finally, as the public value literature recognizes, there is a multistakeholder co-creation of value that involves more than just public managerial effort (see Osbourne, 2020; Bracci et al., 2019; Chohan, 2020c). In Pakistan’s case, the role of civil society (see also Legutko-Kobus, 2018) cannot be downplayed in filling the policy capacity shortcomings and in realizing the policy goals stipulated by the government.
Notwithstanding these limitations, the literature on policy mixes may benefit from analyzing how a developing country might pursue its limited policy capacity through a coherent mix to achieve, at least as of this writing, a comparative success (see also Figure 1) in the COVID-19 pandemic. In that regard, this article’s assertion rests on the fact that those developing countries can adjust sound policy responses to pandemic conditions, despite their resource constraints, by calibrating extant policy instruments and mobilizing new ones within a coherent policy mix.
Author Contributions
The author confirms being the sole contributor of this work and has approved it for publication.
Conflict of Interest
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
ADB (Asian Development Bank) (2020). Proposed Loan and Administration of Grant to Islamic Republic of Pakistan: Emergency Assistance for Fighting the COVID-19 Pandemic. Manila: ADB. Project Number: 54181–001, https://www.adb.org/sites/default/files/project-documents/54181/54181-001-rrp-en.pdf (accessed: 20.07.2021).
Adolph, C., Amano, K., Bang-Jensen, B., Fullman, N., & Wilkerson, J. (2021). Pandemic politics: Timing state-level social distancing responses to COVID-19. Journal of Health Politics, Policy and Law, 46 (2): 211–233.
Ahmed, S. H. (2020, Feb 11). Pakistan’s economy battling a host of challenges. Express Tribune.
Ansell, C., Boin., A., & Keller, A. (2010). Managing Transboundary Crises: Identifying the Building Blocks of an Effective Response System. Journal of Contingencies and Crisis Management 18 (4): 195–207.
Ansell, C., Sørensen, E., & Torfing, J. (2020). The COVID-19 Pandemic as a Game Changer for Public Administration and Leadership? The Need for Robust Governance Responses to Turbulent Problems. Public Management Review 23 (7): 949–960.
Anthony, C., Thomas, T. J., Berg, B. M., Burke, R. V., & Upperman, J. S. (2017). Factors associated with preparedness of the US healthcare system to respond to a pediatric surge during an infectious disease pandemic: Is our nation prepared? American Journal of Disaster Medicine, 12 (4): 203–226.
Ashfaq, M., & Bashir, M. (2020). Pakistan: making a “COVID budget” in a struggling economy. Journal of Public Budgeting, Accounting & Financial Management, 33 (1): 69–77.
Ashford, N. A., Hall, R. P., Arango-Quiroga, J., Metaxas, K. A., & Showalter, A. L. (2020). Addressing inequality: the first step beyond COVID-19 and towards sustainability. Sustainability, 12 (13): 5404.
Błędowski, P. (2014). Polityka społeczna jako specjalność nauk o polityce publicznej – próba charakterystyki. Studia z Polityki Publicznej, 3 (3): 9–23.
Bosi, S., Camacho, C., & Desmarchelier, D. (2021). Optimal lockdown in altruistic economies. Journal of Mathematical Economics, 93: 102488.
Byszewski, G. (2018). Wprowadzenie sieci szpitali z punktu widzenia polityki publicznej. Studia z Polityki Publicznej, 18 (2): 25–36.
Capano, G., & Howlett, M. (2020). The knowns and unknowns of policy instrument analysis: Policy tools and the current research agenda on policy mixes. Sage Open, 10 (1): 1–21.
Capano, G., Howlett, M., Jarvis, D. S., Ramesh, M., Goyal, N. (2020). Mobilizing policy (in) capacity to fight COVID-19: Understanding variations in state responses. Policy and Society, 39 (3): 285–308.
Capano, G., & Woo, J. J. (2017). Resilience and robustness in policy design: A critical appraisal. Policy Sciences, 50 (3): 399–426.
Chapman, R. (2003). A policy mix for environmentally sustainable development-learning from the Dutch experience. New Zealand Journal of Environmental Law, 7: 29.
Chohan, U. W. (2019). Public value and budgeting: International perspectives. Abingdon, OX: Routledge.
Chohan, U. W. (2020a). The Lives or Livelihoods? The Coronavirus Dilemma for Administrations. CASS Working Papers on Economics and National Affairs. Islamabad: CASS. Working Paper ID: EC021UC.
Chohan, U. W. (2020b). Forecasting the economic impact of coronavirus on developing countries: case of Pakistan. CASS Working Papers on Economics and National Affairs. Islamabad: CASS. Working Paper ID: EC016UC.
Chohan, U. W. (2020c, Sept 1). Coronavirus v. Pakistan: Early Successes in the Epidemiological Battle. CASS, https://casstt.com/post/coronavirus-v-pakistan-early-successes-in-the-epidemiological-battle/247 (accessed: 20.07.2021).
Chohan, U. W. (2020d). Modern Monetary Theory (MMT): A General Introduction. CASS Working Papers on Economics and National Affairs. Islamabad: CASS. Working Paper ID: EC017UC.
Chohan, U. W. (2021). Coronavirus & Vaccine Nationalism. CASS Working Papers on Economics and National Affairs. Islamabad: CASS. Working Article ID: EC030UC.
Chohan, U. W. (2022). The return of keynesianism? exploring path dependency and ideational change in post-covid fiscal policy. Policy and Society, 41 (1): 68–82. DOI: 10.1093/polsoc/puab013.
Daugbjerg, C. (2009). Sequencing in public policy: The evolution of the CAP over a decade. Journal of European Public Policy, 16 (2): 395–411.
Davis, G. (2000). Policy capacity and the future of governance. Sydney: Allen & Unwin.
Del Río, P. (2010). Analysing the interactions between renewable energy promotion and energy efficiency support schemes: The impact of different instruments and design elements. Energy Policy, 38 (9): 4978–4989
Dimian, G. C., Apostu, S. A., Vasilescu, M. D., Aceleanu, M I., & Jablonsky, J. (2021). Vulnerability and resilience in health crises. Evidence from European countries. Technological and Economic Development of Economy, 27 (4): 783–810.
Dolowitz, D. P., & Marsh, D. (2000). Learning from abroad: The role of policy transfer in contemporary policy‐making. Governance, 13 (1): 5–23.
Fu, Y., Jin, H., Xiang, H., & Wang, N. (2021). Optimal lockdown policy for vaccination during COVID-19 pandemic. Finance Research Letters, 102123.
Gerard, F., Imbert, C., & Orkin, K. (2020). Social protection response to the COVID-19 crisis: options for developing countries. Oxford Review of Economic Policy, 36 (1): S281–S296.
Ghaffar, A., Alanazi, S., Alruwaili, M., Sattar, M. U., Ali, W., Humayun, M., Siddiqui, S. Y., Ahmad, F., & Khan, M. A. (2021). Multi-Stage Intelligent Smart Lockdown using SIR Model to Control COVID 19. Intelligent Automation and Soft Computing, 28 (2): 429–445.
Ghaffar, A., Munir, M., Aziz, O., Alhajj, R., & Sanaullah, A. (2020). An Assessment of the Smart COVID-19 Approach to Lockdown and its Empirical Evidence. Empirical Economic Review, 3 (2): 31–61.
Grabosky, P. (1995). Counterproductive regulation. International Journal of the Sociology of Law, 23: 347–369.
Hafeez, M. (2014). Poor Healthcare in Pakistan. Harvard International Review, 35 (4): 52.
Hall, P. A. (1993). Policy Paradigms, Social Learning, and the State: The Case of Economic Policymaking in Britain. Comparative Politics, 25 (3): 275.
Hartley, K., & Jarvis, D. S. (2020). Policymaking in a low-trust state: legitimacy, state capacity, and responses to COVID-19 in Hong Kong. Policy and Society, 39 (3): 403–423.
Hassan, A., Mahmood, K., & Bukhsh, H. A. (2017). Healthcare system of Pakistan. IJARP, 1 (4): 170–3.
Hennicke, P. (2004). Scenarios for a robust policy mix: The final report of the German study commission on sustainable energy supply. Energy Policy, 32 (15): 1673–1678.
Howlett, M. (1991). Policy instruments, policy styles, and policy implementation: National approaches to theories of instrument choice. Policy Studies Journal, 19 (2): 1–21.
Howlett, M. (2005). What is a policy instrument? Policy tools, policy mixes and policy styles. In: P. Eliadis, M. Hill, Howlett M. (Eds.), Designing Government: From Instruments to Governance (pp. 31–50), Montreal: McGill-Queen’s University Press.
Howlett, M. (2011). Designing public policies: Principles and instruments. Abingdon, OX: Routledge.
Howlett, M., & Del Rio, P. (2015). The parameters of policy portfolios: Verticality and horizontality in design spaces and their consequences for policy mix formulation. Environment and Planning C: Government and Policy, 33 (5): 1233–1245
Howlett, M., & Rayner, J. (2007). Design principles for policy mixes: Cohesion and coherence in ‘new governance arrangements’. Policy and Society, 26 (4): 1–18.
Hussain, Y., Muhammad, K., Umer, M. F., Omarkhail, A., Khan, S., Kamran, M., Rashid, H., & Khan, Z. (2021). Coronavirus disease 2019 in 5 neighboring limited-resource countries: A financial and health threat. Value in Health Regional Issues, 24: 114–116.
IMF (International Monetary Fund) (2021). Fiscal Monitor: Database of Country Fiscal Measures in Response to the COVID-19 Pandemic. Washington, DC: IMF.
Ittefaq, M., Hussain, S. A., & Fatima, M. (2020). COVID-19 and social-politics of medical misinformation on social media in Pakistan. Media Asia, 47 (1-2): 75–80.
Jabeen, N., Jadoon, Z. I., Mubashar, U. E., & Salman, Y. (2016). Revisiting Public Policy Making Process and Strategies in Pakistan: A Governance Perspective. South Asian Studies, 31 (2): 17–26.
Johns Hopkins University (2021). Johns Hopkins Coronavirus Research Centre. Database. https://coronavirus.jhu.edu/map.html (accessed: 20.07.2021).
Kern, F., & Howlett, M. (2009). Implementing transition management as policy reforms: A case study of the Dutch energy sector. Policy Sciences, 42 (4): 391–408.
Khalid, A., & Ali, S. (2020). COVID-19 and its Challenges for the Healthcare System in Pakistan. Asian Bioethics Review, 12 (4): 551–564.
Knill, C., Steinbacher, C., & Steinebach, Y. (2021). Balancing Trade‐Offs between Policy Responsiveness and Effectiveness: The Impact of Vertical Policy‐Process Integration on Policy Accumulation. Public Administration Review, 81 (1): 157–160.
Koontz, T. M., & Thomas, C. W. (2012). Measuring the performance of public-private partnerships: A systematic method for distinguishing outputs from outcomes. Public Performance & Management Review, 35 (4): 769–786.
Lee, S., Hwang, C., & Moon, M. J. (2020). Policy learning and crisis policy-making: Quadruple-loop learning and COVID-19 responses in South Korea. Policy and Society, 39 (3): 363–381.
Legutko-Kobus, P. (2018). Partycypacja jako element programowania rozwoju lokalnego. Studia z Polityki Publicznej, 19 (3): 45–58.
Mangwat R. (2020, June 4). New algorithm shows alarming number of COVID-19 deaths in Pakistan by August 10. GEO TV.
Maor, M. (2019). Strategic policy overreaction as a risky policy investment. International Review of Public Policy, 1 (1): 46–64.
May, P. J., Sapotichne, J., & Workman, S. (2006). Policy coherence and policy domains. Policy Studies Journal, 34 (3): 381–403
Mei, C. (2020). Policy style, consistency and the effectiveness of the policy mix in China’s fight against COVID-19. Policy and Society, 39 (3): 309–325.
Migone, A. R. (2020). Trust, but customize: Federalism’s impact on the Canadian COVID-19 response. Policy and Society, 39 (3): 382–402.
MNHS (Ministry of National Health Services) (2020). National Action Plan for Corona virus disease (COVID-19) Pakistan. Islamabad: Ministry of National Health Services, Regulation and Coordination Division, https://www.nih.org.pk/wp-content/uploads/2020/03/COVID-19-NAP-V2-13-March-2020.pdf (accessed: 20.07.2021).
Moore, M., & Khagram, S. (2004). On creating public value: What business might learn from government about strategic management. Harvard Kennedy School, Cambridge, MA, http://www.innovations.harvard.edu/creating-public-value-what-business-might-learn-government-about-strategic-management (accessed: 20.07.2021).
Nair, S., & Howlett, M. (2017). Policy myopia as a source of policy failure: Adaptation and policy learning under deep uncertainty. Policy & Politics, 45 (1): 103–118.
NCOC (National Command and Operation Centre) (2020). About Us, https://ncoc.gov.pk/ (accessed: 20.07.2021).
O’Neill, A. (2021). Literacy rate in Pakistan. Statista. https://www.statista.com/statistics/572781/literacy-rate-in-pakistan/ (accessed: 20.07.2021).
Osborne, S. P. (2020). Public Service Logic: Creating Value for Public Service Users, Citizens, and Society Through Public Service Delivery. Abingdon, OX: Routledge.
Osman, F. A. (2002). Public policy making: theories and their implications in developing countries. Asian Affairs, 24 (3): 37–52.
Peter, O. J., Qureshi, S., Yusuf, A., Al-Shomrani, M., & Idowu, A. A. (2021). A new mathematical model of COVID-19 using real data from Pakistan. Results in Physics, 24 (4): 1040–1098.
Peters, B. Guy. (2015). Pursuing Horizontal Management: The Politics of Public Sector Coordination. Kansas City, MO: Lawrence University Press of Kansas.
Preston, L. E., & Post, J. E. (1981). Private management and public policy. California Management Review, 23 (3): 56–62.
Pytlik, B. (2017). Budżet partycypacyjny w Polsce. Ewolucja i dylematy. Studia z Polityki Publicznej, 13 (1): 103–122.
Rasul, G. (2020). A framework for improving policy priorities in managing COVID-19 challenges in developing countries. Frontiers in Public Health, 8 (4): 58–61.
Rocco, P., Béland, D., & Waddan, A. (2020). Stuck in neutral? Federalism, policy instruments, and counter-cyclical responses to COVID-19 in the United States. Policy and Society, 39 (3): 458–477.
Rogge, K. S., & Reichardt, K. (2016). Policy mixes for sustainability transitions: An extended concept and framework for analysis. Research Policy, 45 (8): 1620–1635.
RSP (Rural Support Network Program) (2020). Pakistan’s rural communities fight against Covid-19, http://www.RSP.org/index.php/pakistans-rural-communities-fight-covid-19/ (accessed: 20.07.2021).
Saeed, U., Sherdil, K., Ashraf, U., Younas, I., Butt, H. J., & Ahmad, S. R. (2021). Identification of potential lockdown areas during COVID-19 transmission in Punjab, Pakistan. Public Health, 190: 42–51.
Safdar, A. & Chohan, U. W. (2020). What Ails Pakistan’s Economy? The Problems beyond Coronavirus. CASS Working Papers on Economics & National Affairs, Working Paper ID: EC019ASUC.
Shah, P. T., & Xing, L. (2020). Puzzling increase and decrease in COVID-19 cases in Pakistan. New Microbes and New Infections, 38 (10): 91–93.
Shakir, R., & Qadri, S. (2015). Public Policy Analysis under Military Governance in Pakistan: A Comparative Study of Two Contrasting Regimes. Public Policy, 5 (10): 48–54.
Sharomi, O., & Malik, T. (2017). Optimal control in epidemiology. Annals of Operations Research, 251 (1–2): 55–71.
Shi, W. W., & Tan, Y. S. (2012). Transmission dynamics and optimal control of an influenza model with quarantine and treatment. International Journal of Biomathematics, 5 (03): 1260011.
Syeda, M. H. (2015). Making an impact analysis of social protection programs in Pakistan. Journal of the Research Society of Pakistan, 52 (1): 201–210.
Szarfenberg, R. (2015). Konkretyzacja i koordynacja celów polityki publicznej w wielopoziomowym rządzeniu. Przykład celu Unii Europejskiej w zakresie ubóstwa. Studia z Polityki Publicznej, 6 (2): 41–56.
The Economist (2021). Global Normalcy Index, https://www.economist.com/graphic-detail/tracking-the-return-to-normalcy-after-covid-19 (accessed: 20.07.2021).
Tosun, J., & Lang, A. (2017). Policy Integration: Mapping the Different Concepts. Policy Studies, 38 (6): 553–570.
Trein, P. (2017). Coevolution of Policy Sectors: A Comparative Analysis of Healthcare and Public Health. Public Administration, 95 (3): 744–58.
WHO (World Health Organization) (2020). How polio personnel are pivoting against COVID- 19. Geneva: WHO, https://www.who.int/news-room/feature-stories/detail/how-polio-personnel-are-pivoting-against-covid-19 (accessed: 20.07.2021).
Whoriskey, P., MacMillan, D., & O’Connell, J. (2020, Oct 5). ‘Doomed to fail’: Why a $ 4 trillion bailout couldn’t revive the American economy. Washington Post, https://www.washingtonpost.com/graphics/2020/business/coronavirus-bailout-spending/ (accessed: 20.07.2021).
Woo, J. J. (2020). Policy capacity and Singapore’s response to the COVID-19 pandemic. Policy and Society, 39 (3): 345–362.
Wu, X., Ramesh, M., & Howlett, M. (2015). Policy capacity: A conceptual framework for understanding policy competences and capabilities. Policy and Society, 34 (3–4): 165–171.
Yang, K. (2020). Unprecedented challenges, familiar paradoxes: COVID-19 and governance in a new normal state of risks. Public Administration Review. 80 (4): 657–664.
Yusufzai, A. (2020). Efforts to eradicate polio virus in Pakistan and Afghanistan. The Lancet Child & Adolescent Health, 4 (1): 17.
Unless stated otherwise, all the materials are available under
the Creative Commons Attribution 4.0 International license.
Some rights reserved to SGH Warsaw School of Economics.
